Cosmetic Surgery Blog
Skin Cancer and Internal Malignancy. Another thing to worry about!

Patients with a history of a none melanoma skin cancer such as basal cell or squamous cell cancer are at higher risk of subsequent basal cell or squamous cell cancers. However a recent study from Korea has suggested that these patient may also be at risk for other types of malignancies such as bone cancer or cervical cancer. This nationwide cohort study, compared 27 259 none melanoma skin cancer patients with 54 518 matched controls without skin cancer, Patients were followed for 8 years to observe the development of any internal malignancies after a diagnosis of skin cancer.
The risk was significantly higher in the patients with skin cancer. Bone cancer showed the highest risk followed by nasal cavity and larynx , oral cavity and pharynx (HR , anus and anal canal and cervical cancers with risks greater than five-fold higher in none melanoma skin cancer patients compared with the controls.
So now when you get you diagnosis of skin cancer you need to get it treated, take precautions to limit your risk of future skin cancers, monitor your skin carefully for any suspicious lesions, and be aware that you may be at higher risk for several other unrelated malignancies!
However these results were from a relatively none diverse patient population and still need to be confirmed by other studies. How much “extra” risk of these internal malignancies Americans with skin cancer will have is yet to be definitively determined.
Article Citation
Journal of the European Academy of Dermatology and Venereology: JEADV
Non-Melanoma Skin Cancer as a Clinical Marker for Internal Malignancies: A Nationwide Population-Based Cohort Study
J Eur Acad Dermatol Venereol 2019 Sep 08;[EPub Ahead of Print], SJ Yun, JM Bae, H Kim, BC Park, JS Kim, SH Seo, HH Ahn, DY Lee, YC Kim, HJ Park, KY Chung
Younger generation seem to be getting the message about melanoma!

While the overall incidence of melanoma seems to be on the rise, there was a significant lowering in the rate of melanoma in among adolescents (10–19 years of age) and young adults (20–29 years of age). Using registry data, these authors evaluated 988,103 cases of invasive melanoma and found that, the overall incidence of melanoma increased from 200 to 229 cases per million person-years from 2006 to 2015, respectively. However over the same period the incidence among adolescents (10–19 years of age) and young adults (20–29 years of age) significantly declined. Incidence rates of melanoma decreased by an annual percentage change of −3.6% to −5.4% in both males and females in these age ranges. The declining incidence of melanoma among adolescents and young adults may be a result of the efforts promoting sun protective interventions and that messaging having a real impact on the behavior of the younger generation. Lets hope the trend continues!
Age-Specific Incidence of Melanoma in the United States
JAMA Dermatol 2019 Nov 13;[EPub Ahead of Print], KG Paulson, D Gupta, TS Kim, JR Veatch, DR Byrd, S Bhatia, K Wojcik, AG Chapuis, JA Thompson, MM Madeleine, JM Gardner
Sniffing Out Malignant Melanoma

Not for the first time, an article that suggests that dogs can “smell” a melanoma and react to it. A 43 year old women presented to her doctor for evaluation of a mole on her back that had been present since childhood. She described how recently her 2 year old rescue dog had been frequently sniffing the mole and would subsequently get agitated and try to scratch and bite the lesion. A biopsy was taken and proved the lesion to be a melanoma.
Malignant melanocytes found in melanomas release volatile organic compounds that can differ from those released by normal melanocytes that make up normal moles. Volatile organic compounds released at the skin’s surface can be detected by various methods, including canine olfaction; therefore, unusual canine behavior toward skin lesions should not be ignored. If you dog doesn’t like the smell of it your dermatologist may not like the look of it!
Citation:
Cutis; Cutaneous Medicine for the Practitioner
Sniffing Out Malignant Melanoma: A Case of Canine Olfactory Detection
Cutis 2019 Sep 02;104(03)E4-E6, R Srivastava, JJ John, C Reilly, AM John, BK Rao
Mohs for Melanoma

Fredrick Mohs, the founder of the technique that caries his name, used his method for the treatment of Melanoma as well as basal cell and squamous cell carcinomas. Since then Mohs surgery has become the gold standard for treating none melanoma skin cancer. However more recent data is confirming the fact that Mohs surgery can work as well if not better than traditional surgery in the management of melanoma as well. In a recent retrospective study looked at the outcome of over 50,000 melanomas of the head and neck treated with either traditional wide excision or Mohs surgery. After controlling for potential confounding variables, patients treated with MMS were more likely to survive after 5-years than patients treated with wide local excision. Certainly it is time to seriously consider Mohs surgery for melanomas of the head and neck as well as the usual none melanoma skin cancers.
Citation:
Journal of the American Academy of Dermatology
Improved Overall Survival of Melanoma of the Head and Neck Treated With Mohs Micrographic Surgery Versus Wide Local Excision
J Am Acad Dermatol 2019 Aug 29;[EPub Ahead of Print], J Hanson, A Demer, W Liszewski, N Foman, I Maher
Sex Matters: Men With Melanoma Have a Worse Prognosis Than Women

We already know that men tend to present to the doctor with melanomas that are on average more advanced than the melanomas found in women. However, a recent study from the Netherlands found that even when you take into account this difference, men overall have a worse prognosis than women as far as melanoma goes. That means even if the melanomas appear to be at the same stage, if it is on a man there is a higher risk it will result in death than if the same melanoma was on a woman. The reasons for this difference are not clear but possibly could be related to androgen levels. Whatever the cause it highlights the need to subdivide different patients as well as different melanomas to get a more accurate prognosis and so guide treatment as well as education and preventative strategies. Certainly it should be a wake up call to men how may be reluctant to visit their doctor for a skin cancer screening exam.
Article Citation:
Journal of the European Academy of Dermatology and Venereology: JEADV
Sex Matters: Men With Melanoma Have a Worse Prognosis Than Women
J Eur Acad Dermatol Venereol 2019 Jun 27;[EPub Ahead of Print], MA El Sharouni, AJ Witkamp, V Sigurdsson, PJ van Diest, MWJ Louwman, NA Kukutsch
A biopsy may not give the whole story

Surely when you get a final pathology report from a biopsy you have a definitive diagnosis? Well not always. While diagnosing a basal cell carcinoma or squamous cell cancer is usually pretty straightforward, the biopsy is only a sample of a larger tumor. So what is seen on the biopsy may not be identical to what is present in the rest of the tumor. This is not to say that what was diagnosed a basal cell cancer could really be a melanoma or anything like that. However there are many different sub-types of basal cell and squamous cell cancer, and some of them are a lot more aggressive than others. So while the biopsy may show a non- aggressive sub-type a more complete analysis may show areas of more aggressive disease that would require a wider surgical margin to remove. This is another instance where Mohs surgery seems to be beneficial. In a recently published study it was found that during Mohs surgery for basal and squamous cell cancers the Mohs surgeon found evidence of more aggressive disease more than 10% of the time. These cases were more likely to need more Mohs stages. Had an other treatment modality been used it is likely that this aggressive component of the tumor would be missed and some cancer be unwittingly left behind.
Citation:
Histopathologic upgrading of nonmelanoma skin cancer at the time of Mohs micrographic surgery: A prospective review
Rachel L. Kyllo, MDa, Karl W. Staser, MD, PhDa, Ilana Rosman, MDa,b, M. Laurin Council, MDa,c, Eva A. Hurst, MD
JAAD August 2019 Volume 81, Issue 2, Pages 541–547
Too Much or Too Little?

Mohs surgery is considered the gold standard for the treatment of most skin cancers. However, not all Mohs surgeons perform the procedure the same way.
When performing Mohs micrographic surgery for the treatment of skin cancer, the surgeon starts by removing what he/she estimates to be “just enough” tissue to clear the cancer. Obviously, you do not want your surgeon to take too much and create a larger hole than was needed. But at the same time, if he/she takes too little, extra stages will be needed until the cancer is cleared.
Some cancers have subclinical extensions (like the roots of a weed) that go well beyond what is obvious on the surface. In these cases, a Mohs surgeon will need to perform multiple stages to get clear margins. In other cases, the cancer is more limited and a single stage is all that is needed.
So, on average, how many stages of Mohs should a Mohs surgeon be performing overall? A recent study published in JAMA Dermatology indicated that the average rate should be between 1.4 and 2.4 stages.
Many cases only require a single stage, while others need multiple stages. The ability to take the appropriate amount of tissue with each stage is not an exact science. It is something that comes through training, experience, and judgement.
Dr. Ralph Massey is a world-class cosmetic and skin-cancer surgeon. He completed his fellowship in Mohs micrographic and cosmetic surgery at Columbia University and served as an assistant clinical professor at both Columbia University and UCLA.
In addition, he has enjoyed years of experience and is now recognized by many as the “go to” surgeon for skin-cancer management. Contact our office today and set up a consultation to find out more about Mohs surgery and what it can do for you.
Citation:
Outlier Practice Patterns in Mohs Micrographic Surgery Defining the Problem and a Proposed Solution
Aravind Krishnan, BA1; Tim Xu, MPP1; Susan Hutfless, PhD2,3; et al and the American College of Mohs Surgery Improving Wisely Study Group
JAMA Dermatol. 2017;153(6):565-570.
You don’t need to be White to get Skin Cancer!

While the vast majority of skin cancers occur in whites, nonwhites are not immune. A recent retrospective study showed that in whites and Hispanics basal cell carcinoma was the most frequent skin cancer diagnosis, however in blacks and Asians, the potentially more ominous squamous cell carcinoma (SCC) was more common. Also, as opposed to whites, the majority of the SCCs in blacks occurred in sun-protected areas (in particular, the anogenital region). Many of these may be related to human papilloma virus (warts), a small subset of which are know to be carcinogenic. Its important that dermatologists be aware of the potential for skin cancer in these populations, and when performing skin cancer screening they should examine sun protected areas as well as the exposed parts.
Citation
Journal of the American Academy of Dermatology
Risk Factors for Keratinocyte Carcinoma Skin Cancer in Nonwhite Individuals: A Retrospective Analysis
J Am Acad Dermatol 2019 Jan 28;[EPub Ahead of Print], KS Nadhan, CL Chung, EM Buchanan, C Shaver, S Shipman, RM Allawh, ML Hoffman, G Lim, M Abdelmalek, CA Cusack
Melanomas are not always dark
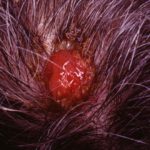
Most people would be concerned about a mole that became very dark. Any we know that the vast majority of melanomas are pigmented, that is they look black, brown or maybe dark blue and often more than one shade or color. However “amelanotic” melanomas are uncommon form of melanomas that have no pigmentation. They may appear as a pink bump or patch, or sometime a raw looking pink nodule. A recent study highlight why we need to be especially vigilant in looking out for these. In this retrospective study it was found that amelanotic melanomas are more likely to be misdiagnosed and diagnosed at an older age with more aggressive features and shorter survival. More awareness and a lower threshold for biopsy may help detect these potentially deadly lesion before it is too late.
Citation:
Journal of the American Academy of Dermatology
Clinicopathologic, Misdiagnosis and Survival Differences Between Clinically Amelanotic Melanomas and Pigmented Melanomas
J Am Acad Dermatol 2019 Jan 14;[EPub Ahead of Print], LC Strazzulla, X Li, K Zhu, JP Okhovat, SJ Lee, CC Kim
Extremity moles linked to increase skin cancer risk.

The association between having lots of atypical moles all over your body and subsequent melanoma is well established. In a more recent prospective study the risk of moles on the extremities (arms and legs) was specifically looked at. Patients with more than 15 moles on their arms and legs had an almost 3 times risk for melanoma. These melanomas could occur anywhere on the body not just on the extremities, but having more than 15 extremity nevi (moles) identified patients who were at heightened risk.(There was also a small increase risk for basal cell carcinoma also noted but no increase risk of squamous cell cancer in this population). So take close look at your arms and legs and see if you can count to 15, it may be time to get checked!
Citation:
Journal of the American Academy of Dermatology 2019
Extremity Nevus Count Is an Independent Risk Factor for Basal Cell Carcinoma and Melanoma, but Not Squamous Cell Carcinoma
J Am Acad Dermatol 2019 Jan 31;[EPub Ahead of Print], EX Wei, X Li, H Nan